Homo Candidus and Longetivity

- I. Why This Matters
- The Receptor-to-Condition Map
- Reproductive and Endocrine Interface
- Autonomic and Cardiovascular Interface
- Neurological and Neuromodulatory Interface
- Gastrointestinal Interface
- Immune Interface
- Metabolic Interface
- Urogenital and Pain Interface
- Addiction and Reward Interface
- Obesity and Weight Regulation Interface
- What This Number Represents
- Mortality
- How Medicine Changes
- The Obligate Partner
- Homo Candidus: What the Framework Gives Us
- A Note from the Architect
- The Receptor-to-Condition Map
Original Article with References at: https://doi.org/10.5281/zenodo.19488041
[Hello, readers. First, hit that share button if you make it halfway through - I think you might. Second, subscribe, I have an endless list of subjects to cover. Third, thanks for reading. Finally, this article should give you hope for humanity. Yes, this is a Fourth Turning, and we are not making the right decisions as a species, but there is something that can bring us all together. What if we were smarter, could live longer, and be healthier simply by taking advantage of what we already have inside us? Come along…find out why and how…]
I. Why This Matters
What do we gain from understanding the true nature of Candida Albicans? Are we searching for a better way to kill it? Do we think we can change it through some biological re-engineering? Are we just describing for the first time all the ontological features of a novel disease? No.
The framework described in this series does not propose a novel disease. It proposes that a single organism, already resident in the majority of the human population, already documented to sense, modulate, or compete for substrates across at least thirteen confirmed host signaling systems, may be the common upstream variable in dozens of conditions that medicine currently treats as separate diseases with unknown etiology.
This is not speculation. It is a mechanical consequence of the receptor inventory.
First, we should review the inventory of tools in it’s toolbox. Then we can discuss the implications and the only real path forward. [I’m here, but we are just warming up]
The Receptor-to-Condition Map
Each confirmed sensing or modulatory interface described in Paper A (Craddock, 2026a) connects the organism to host systems whose dysfunction defines entire disease categories. The conditions listed below share three features: (1) their textbook descriptions include “unknown etiology,” “idiopathic,” or “multifactorial”; (2) they involve signaling systems the organism has documented access to; and (3) they are currently treated as independent diagnoses with separate research funding, clinical guidelines, and pharmaceutical pipelines.
Reproductive and Endocrine Interface
Organism access: Estrogen (Ebp1), LH/hCG (high-affinity binding sites), androgens (sterol-binding proteins), corticosteroids (corticosteroid-binding protein), plus indirect governance of FSH, TSH, prolactin, and growth hormone via pituitary perfusion and ECS modulation.
Conditions currently classified as separate diseases:**
Polycystic ovary syndrome (PCOS). Endometriosis. Unexplained infertility. Premenstrual dysphoric disorder. Recurrent pregnancy loss. Early menopause. Gynecomastia. Hypogonadism. Hypothyroidism/hyperthyroidism of unclear origin. Cushing-adjacent presentations. Addison-adjacent presentations. Amenorrhea. Dysmenorrhea.
Current U.S. spending: Endometriosis alone carries an estimated annual burden of $69.4 billion in direct and indirect costs. PCOS affects 6–12% of reproductive-age women. Infertility treatment represents a multi-billion-dollar industry built on conditions the organism’s receptor inventory could explain mechanistically.
Autonomic and Cardiovascular Interface
Organism access: Muscarinic acetylcholine receptor (parasympathetic arm, direct). ECS-mediated catecholamine governance (sympathetic arm, indirect). Angiotensin II interaction via RAAS. Pituitary-mediated ADH modulation.
Conditions currently classified as separate diseases:**
Postural orthostatic tachycardia syndrome (POTS). Dysautonomia. Inappropriate sinus tachycardia. Idiopathic hypotension. Raynaud’s phenomenon. Vasovagal syncope. Neurogenic bladder. Idiopathic hyperhydrosis.
Neurological and Neuromodulatory Interface
Organism access: Dopaminergic interface (Gpr1/clozapine response). Tryptophan/kynurenine rerouting (serotonin depletion). ECS tone modulation (CB1/CB2 governance). Histamine release via mast cell degranulation (mannan/beta-glucan). ATP/purinergic signaling via candidalysin. Melatonin sensing.
Conditions currently classified as separate diseases:**
Major depressive disorder. Generalized anxiety disorder. ADHD. Autism-adjacent sensory and behavioral presentations. Insomnia. Idiopathic hypersomnia. Restless leg syndrome. Fibromyalgia. Chronic fatigue syndrome/ME. Migraine. Cluster headache. Chronic pain syndromes. Brain fog.
Current U.S. spending: Major depressive disorder alone carried an estimated economic burden of $326.2 billion in 2018, growing at 38% per decade. Mental illness broadly costs the U.S. economy an estimated $282 billion annually. Fibromyalgia adds $16–20 billion. ME/CFS adds $18–24 billion in direct and indirect costs. Migraine adds $36–78 billion depending on methodology. These figures are additive because each condition is funded, researched, and treated independently.
Gastrointestinal Interface
Organism access: Hgt4 glucose sensing (calibrated to human blood glucose). Gut colonization and pH engineering (Rim101, alkalinization). Arachidonic acid competition at the PGE2/endocannabinoid branch point. Peptide transport system (10 dedicated transporters). CB1 receptor density maintenance in gut epithelium. Microbiome management.
Conditions currently classified as separate diseases:**
Irritable bowel syndrome (IBS). Small intestinal bacterial overgrowth (SIBO). Gastroparesis. Functional dyspepsia. Cyclic vomiting syndrome. Cannabinoid hyperemesis syndrome (CHS). Eosinophilic esophagitis. Non-celiac gluten sensitivity. Chronic nausea of unknown origin. Histamine intolerance.
Immune Interface
Organism access: Th2 skewing via PGE2. Dendritic cell suppression via farnesol. LILR engagement via Ece1 peptides. Mast cell degranulation via cell wall components. Beta-glucan masking. Complement evasion via Factor H binding.
Conditions currently classified as separate diseases:**
Mast cell activation syndrome. Chronic urticaria. Recurrent infections of unclear origin. Lupus-adjacent presentations. Multiple sclerosis-adjacent presentations. Psoriasis. Eczema/atopic dermatitis. Inflammatory bowel disease. Sarcoidosis. Chronic sinusitis. Interstitial cystitis. Chronic prostatitis.
Current U.S. spending: Autoimmune diseases collectively exceed $100 billion annually in direct healthcare costs, with projections reaching $180 billion by 2025 for 29 tracked diseases alone. This figure is widely acknowledged as a significant undercount because only 7 of over 100 recognized autoimmune conditions have been rigorously costed.
Metabolic Interface
Organism access: Glucose consumption and Hgt4-mediated set point maintenance. Arachidonic acid substrate competition. Tryptophan diversion. Na+/K+-ATPase reversal. Ketone and lactate utilization. Oxygen tension sensing.
Conditions currently classified as separate diseases:**
Type 2 diabetes (organism-managed glucose floor confounding insulin resistance diagnosis). Metabolic syndrome. Unexplained weight gain or loss. Reactive hypoglycemia. Non-alcoholic fatty liver disease. Eating disorders (organism-driven craving and satiety signal manipulation).
Urogenital and Pain Interface
Organism access: PGE2 production. Candidalysin-mediated tissue engagement. Mast cell degranulation. ECS tone disruption. Purinergic signaling.
Conditions currently classified as separate diseases:**
Interstitial cystitis/painful bladder syndrome. Chronic pelvic pain. Vulvodynia. Chronic prostatitis/chronic pelvic pain syndrome. Nocturnal enuresis (bedwetting). Endometriosis-associated pain.
Addiction and Reward Interface
Organism access: Dopaminergic signaling (Gpr1 responds to dopamine receptor antagonist clozapine). Serotonin depletion via tryptophan/kynurenine diversion. Endocannabinoid tone disruption through arachidonic acid substrate competition and CB1 receptor density maintenance. Histamine release via mast cell degranulation. GABA-adjacent interactions (benzodiazepine responsiveness documented in CHS pharmacology). Purinergic signaling via candidalysin-mediated ATP efflux. Endogenous ethanol production via fermentation. The organism has documented access to every major reward and reinforcement pathway in the human brain.
Conditions currently classified as separate diseases:**
Alcohol use disorder. Opioid use disorder. Stimulant use disorder. Cannabis use disorder. Nicotine dependence. Behavioral addictions (gambling, compulsive eating). Substance-induced mood disorders.
Current U.S. spending: Substance abuse costs the United States over $740 billion annually: alcohol ($249 billion), tobacco ($300 billion), and illicit and prescription drugs ($193 billion combined). The federal drug control budget alone was $44.5 billion in 2024. Nearly 48.5 million Americans aged 12 and older met criteria for a substance use disorder in 2023. The “hijacked reward circuit” model of addiction is correct — it misidentifies who is doing the hijacking. The organism modulates the same dopaminergic, serotonergic, and endocannabinoid pathways that addiction neuroscience has identified as central to compulsive substance use. Alcohol is not merely a substance the host consumes; it is a fermentation product and a direct carbon source for the organism. The host’s craving may not be entirely the host’s.
Obesity and Weight Regulation Interface
Organism access: Glucose consumption and Hgt4-mediated metabolic governance. ECS tone modulation (appetite and satiety signaling via CB1). Dopaminergic reward pathway access (Gpr1). Serotonin depletion via tryptophan diversion (serotonin regulates satiety). Lipid metabolism modulation (sterol requirements for membrane construction). Insulin signaling interference. The organism benefits from substrate accumulation in the host and has the signaling access to drive it.
Conditions currently classified as separate diseases:**
Obesity (all classes). Metabolic syndrome. Binge eating disorder. Non-alcoholic fatty liver disease.
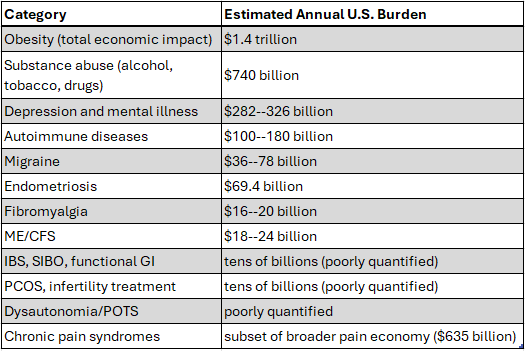
Current U.S. spending: The total economic impact of obesity in the United States exceeds $1.4 trillion annually, including $260 billion in direct medical costs and over \(400 billion in employer costs from reduced productivity, absenteeism, and disability. Forty percent of American adults are obese. The anti-obesity pharmaceutical market, including the GLP-1 receptor agonists currently generating tens of billions in annual revenue, is treating a downstream consequence of organism-managed appetite and metabolic signaling operating without the periodic reset the saline oscillation provides. The organism drives substrate accumulation because it benefits from substrate availability. The host gains weight because the organism’s metabolic program is running unchecked. ## **The Aggregate** Conservative summation of available U.S. cost estimates across these categories: [s_!E6eX!,w_1456,c_limit,f_auto,q_auto:good,fl_progressive:steep/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2Fc4d06611-8958-42d2-afd9-22b15ca1f8ff_525x351.png)](https://substackcdn.com/image/fetch/$s_!E6eX!,f_auto,q_auto:good,fl_progressive:steep/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2Fc4d06611-8958-42d2-afd9-22b15ca1f8ff_525x351.png)
{kind=link}
These are not competing estimates. They are separate line items in separate budgets funding separate research programs investigating separate diseases—each of which involves signaling systems a single organism has documented access to.
The total exceeds $2 trillion annually in the United States alone, and this figure excludes the conditions for which no rigorous cost-of-illness studies exist (POTS, dysautonomia, histamine intolerance, cyclic vomiting syndrome, chronic prostatitis, vulvodynia, nocturnal enuresis, and others). It represents roughly 40% of all U.S. healthcare spending — $5.3 trillion in 2024 — potentially traceable to a single unexamined upstream variable. [Ch-ching, sounds profitable if you are on the other side of it]
What This Number Represents
This is not a claim that every case of every listed condition is organism-mediated. Colonization density varies. Host genetics vary. Environmental exposures vary. The claim is narrower and more consequential: if the framework is correct, then the majority of conditions on this list share a common upstream variable that current medicine does not test for, does not look for, and has no diagnostic protocol to identify.
The pharmaceutical, diagnostic, and research infrastructure built around these conditions as independent diseases represents the single largest misallocation of medical resources in history—not because the spending is wasteful per se, but because it is aimed at downstream symptoms while the upstream cause remains unexamined.
Mortality
The mortality data are harder to aggregate because most of these conditions kill indirectly—through suicide (depression, chronic pain), through cardiovascular events (dysautonomia, metabolic syndrome, autoimmune vasculitis), through organ failure in advanced cases, or through the accumulated physiological cost of decades of unrecognized organism management. The framework predicts that a significant fraction of deaths currently attributed to “complications of” autoimmune disease, metabolic syndrome, cardiovascular disease, and suicide may trace to the same upstream variable.
[But, there is another side to mortality – longevity…]
How Medicine Changes
If the framework is validated, the consequences cascade through every level of medical practice:
Diagnosis shifts from symptom-cluster pattern recognition to direct assessment of colonization density, organism activity markers, and host-organism signaling state. The diagnostic odyssey—the average 4.5 years and multiple specialists required to diagnose conditions like endometriosis, fibromyalgia, or lupus—collapses to a single investigative framework.
Treatment shifts from managing downstream symptoms (SSRIs for serotonin depletion the organism caused, biologics for immune dysregulation the organism drives, hormone replacement for axes the organism governs) to addressing colonization directly. The $73 billion global autoimmune treatment market and the $26 billion antidepressant market are built on symptom management that leaves the upstream cause untouched.
Research converges. Instead of separate funding streams for migraine, fibromyalgia, IBS, PCOS, depression, and autoimmune disease—each with its own journals, conferences, professional societies, and pharmaceutical pipelines—the relevant science reduces to mycology, host-symbiont signaling, and coevolutionary biology. The 1,300 uncharacterized orphan genes in C. albicans become the most consequential unstudied genome in human medicine.
Prevention becomes possible. If colonization density and organism program advancement can be assessed, intervention before symptom onset becomes feasible—a concept that does not exist in the current framework for any of these conditions except through genetic screening for autoimmune risk factors.
The organism has been in the room for every one of these diagnoses. The question is whether medicine is willing to look at it. [I think we have no choice, let’s discuss…]
The Obligate Partner
The natural response to Section A is: if a single organism is upstream of $2 trillion in annual disease burden, then eliminate the organism. [“Kill it” they said in 1965 after they learned all about it and decided not to tell anyone]
This is the wrong answer. It is also the answer that modern medicine has been inadvertently [?] pursuing for decades, and the results speak for themselves.
Why You Cannot Win by Fighting
Every antifungal intervention produces systemic consequences that medicine documents but does not explain within its current framework. Fluconazole disrupts sterol synthesis — but sterol synthesis is a shared biochemical pathway between the organism and every human cell membrane. Amphotericin B targets ergosterol in fungal membranes — but its nephrotoxicity and cardiotoxicity reflect the collateral damage of attacking a partner whose metabolic infrastructure is interleaved with the host’s. The side effect profiles of antifungal agents are not incidental toxicities. They are the predictable consequences of attacking half of a coupled system.
The pattern extends beyond antifungals. Immunosuppressants prescribed for autoimmune conditions — conditions the framework attributes to organism-driven immune modulation — suppress the immune activity the organism is managing. The result is not resolution. It is a new equilibrium in which both the organism’s management and the host’s defense are degraded, producing the cascading opportunistic infections and secondary complications that define long-term immunosuppressive therapy. Antibiotics prescribed for bacterial infections disrupt the gut microbiome the organism governs as part of its competitive landscape, producing the post-antibiotic dysbiosis and recurrent infection cycles that have become a defining feature of modern medicine. [See Focal Infections 2.0: C. albicans and Dysbiosis]
Medicine is not failing to treat these conditions. It is succeeding at disrupting a system it does not know exists, and documenting the consequences as side effects.
The Logic of Obligate Partnership
The organism that kills its host dies. This is not a philosophical position. It is an evolutionary constraint. A million years of coevolution have selected, at the population level, for organism lineages whose management programs maintain host viability. Organism variants that consumed too aggressively, that advanced their programs too rapidly, that destroyed host organ systems before completing their own reproductive objectives — those lineages ended when their hosts ended. What remains is an organism whose entire computational architecture is oriented toward keeping the host alive and functional for as long as the organism requires.
The inverse is equally binding. A host that eliminates the organism loses every maintenance function the organism provides. After a million years of coupled selection, human physiology is not merely tolerant of the organism’s presence. It is dependent on it. The glucose regulation, immune calibration, cardiovascular governance, cholesterol management, and infection suppression described throughout this framework are not functions the host performs independently with the organism as an unwelcome passenger. They are functions that the coupled system performs together. Remove the organism, and the host must perform them alone, with machinery that has been co-opted, shared, or partially offloaded to the symbiont across evolutionary time.
This is what an ideal symbiont looks like from the perspective of evolutionary game theory. Not an organism that helps by choice. An organism that cannot afford to harm, coupled with a host that cannot afford to eliminate. Neither party can defect. The fitness of each is bound to the fitness of the other.
If the host’s genetics decline — if metabolic function degrades, if immune competence erodes, if organ systems fail — the organism’s environment degrades with them. The organism has every evolutionary incentive to prevent this. If the organism is eliminated — if colonization is eradicated through aggressive antifungal therapy or immune reconstitution — the host loses every maintenance subsidy the organism was providing. The decline that follows is not recovery. It is the unmasking of dependence.
The Only Viable Strategy
There is no therapeutic path that leads through the destruction of the organism to improved host outcomes. The coupled architecture forecloses it. Every attempt to kill the organism harms the host. Every attempt to suppress the organism’s outputs suppresses functions the host requires.
The only strategy that produces improved outcomes is management. Not elimination. Not suppression. Management of the combined condition called Homo Candidus and the phase changes that keep colonization density within the range where the organism’s maintenance functions operate without its pathological outputs overwhelming host compensatory capacity.
This is not a concession. It is the recognition of what the relationship actually is. And it transforms the clinical question from “how do we fight this organism” to “how do we manage this partnership,” — which is the question that leads to everything described in the following section.
You cannot fight this. That is a fool’s errand. It is literally our other half. Sure, you can build a drug that kills some of it – and it will come back new and different and not configured like it was before or worse, just stop doing maintenance and you will get some combination of comorbidities.
Or, you can join it. [“This is the way”]
Homo Candidus: What the Framework Gives Us
The previous section quantified the cost of not knowing. This section describes what becomes possible when the relationship is understood.
The Scale of Current Failure
The United States spent $5.3 trillion on healthcare in 2024, or $15,474 per person. Ninety percent of that spending goes to chronic and mental health conditions. Chronic disease alone is projected to cost the nation $47 trillion over the next fifteen years. This is not a healthcare system. It is a sick care system: an infrastructure built to manage symptoms downstream of causes it has never identified.
The organism described in this framework has documented access to the signaling systems that drive the conditions consuming the majority of that spending. The aggregate annual U.S. cost of conditions plausibly linked to organism activity — depression, autoimmune disease, migraine, endometriosis, fibromyalgia, chronic fatigue, obesity, addiction, metabolic syndrome, dysautonomia, chronic pain, and the functional gastrointestinal disorders — exceeds $2 trillion when obesity ($1.4 trillion in total economic impact) and substance abuse ($740 billion) are included alongside the figures enumerated in Section A.
This is what ignorance costs. Every dollar represents a treatment aimed at a symptom produced by a system no one is examining.
But the Organism Is Not the Enemy
This is the point the framework makes that no other model in medicine currently offers: the organism is not simply causing disease. It is running maintenance. The same capabilities that produce pathology when unrecognized and unmanaged produce extraordinary physiological outcomes when the relationship is understood.
The organism manages cholesterol — it requires host lipids for membrane construction and actively modulates sterol metabolism. It regulates glucose — Hgt4 is calibrated to human blood glucose, and the organism consumes glucose directly, maintaining a floor that prevents the hyperglycemic damage driving the $327 billion annual cost of diabetes. It suppresses bacterial competitors through direct antimicrobial activity, biofilm competition, and immune landscape management — the managed gut barrier described in Paper B represents a functional defense against the enteric pathogens that killed more humans than any other cause for most of evolutionary history. It governs cardiovascular tone through dual autonomic access. It maintains immune surveillance through continuous low-level immune engagement that keeps the adaptive immune system primed.
The conditions that kill the majority of humans in developed nations — cardiovascular disease ($233 billion annually, projected to reach $2 trillion by 2050), diabetes ($327 billion), infection, and cancer (where immune surveillance failure is a primary enabling event) — are all systems the organism actively manages as part of its own survival program. The organism does not want the host to die. A dead host is a dead organism. Every maintenance subroutine it runs is aimed at keeping the host alive long enough for the organism to complete its own program.
The problem is not the organism. The problem is unmanaged program advancement.
The Phase Transitions as Reset
Redacted Science describes the process: the documented phases, pulling colonization density back from levels that produce symptomatic disease to levels that produce managed maintenance. The organism’s own architecture — its bet-hedging, its phenotypic switching, its population-level diversity — means it recovers from each reset [and so does the host]. Each interval between resets is a period of managed physiology, during which the organism is performing the maintenance functions that its coevolutionary architecture was selected to perform. Meanwhile, there are also perks.
The historical pattern is clear. For the majority of the coevolutionary period, saline oscillation created the conditions that progressed Homo Candidus naturally through environmental exposure. The organism and host population cycled together. The conditions listed in Section A — the ones medicine now treats as separate diseases — did not present as chronic conditions because the organism never reached the colonization density at which they manifest. Today’s diseases of are of unmanaged coevolution. They are diseases of forgetting what we are. They are diseases we cause by fighting our own genetic history.
What Homo Candidus Looks Like [Perks]
Homo Candidus is not a new species. It is Homo sapiens with the relationship understood and managed. The organism stays. It has been part of the human platform for over a million years. Its removal is neither feasible nor desirable — its maintenance functions are too deeply integrated into human physiology to disentangle. What changes is management.
A managed Homo Candidus phenotype means:
Metabolic regulation without metabolic disease. The organism manages glucose, cholesterol, and lipid metabolism as part of its own substrate requirements. In a managed state, this produces metabolic parameters that conventional medicine would describe as optimal — without medication, without dietary restriction beyond what the organism’s own glucose management provides, and without the progressive metabolic deterioration that currently drives diabetes, metabolic syndrome, and their downstream cardiovascular consequences.
Immune competence without autoimmune disease. The organism’s continuous low-level immune engagement keeps the adaptive immune system active and calibrated. In a managed state, this produces robust pathogen defense and functioning immune surveillance. It does not produce the Th2-skewed, self-attacking immune dysfunction that occurs when colonization density rises to the point where the organism’s immunomodulatory outputs overwhelm host regulatory capacity. The $180 billion autoimmune disease burden is the cost of an immune system being managed by an organism no one knows is there.
Neurological stability without psychiatric disease. The organism modulates dopamine, serotonin (via tryptophan diversion), endocannabinoid tone, histamine, and GABA-adjacent signaling. In a managed state, these modulations produce stable mood, regulated sleep, appropriate reward signaling, and cognitive function that the case study describes as enhanced, not impaired. Depression, anxiety, ADHD, and the constellation of neuromodulatory conditions listed in Section A are what these same modulations produce when colonization density advances past the managed threshold. [You can still get depressed and anxious, but go for a run and you feel great]
Cardiovascular efficiency. Dual autonomic access — parasympathetic via the muscarinic receptor, sympathetic via ECS-mediated catecholamine governance — produces cardiovascular regulation that in the managed case study produced the fastest heart rate recovery to baseline in standardized workplace fitness testing. This is the same system that produces POTS, dysautonomia, and idiopathic arrhythmias when unmanaged.
Infection resistance. The managed gut barrier, the organism’s suppression of bacterial competitors, and continuous immune priming produce a host that is substantially more resistant to bacterial infection than one without an active symbiont. Dysentery, the leading cause of death for most of human history, is the clearest example: a managed gut barrier with active organism governance of the intestinal environment is a gut that enteric pathogens cannot easily breach. The framework predicts that Homo Candidus populations had lower mortality from infectious disease than populations without the oscillation — and that this advantage was one of the primary selection pressures that made the relationship obligate.
Obesity resolution. The organism consumes glucose, manages lipid metabolism, and governs satiety and craving signaling through the ECS, dopaminergic, and serotonergic interfaces. Obesity — which carries a total economic impact exceeding $1.4 trillion annually in the United States and affects 40% of the adult population — is, within this framework, a downstream consequence of organism-managed metabolic and appetite signaling operating without the periodic reset that the saline oscillation provides. The organism drives substrate accumulation because it benefits from substrate availability. The host gains weight because the organism’s program is running unchecked. Managed oscillation intervals reset this accumulation cycle. The $30 billion anti-obesity pharmaceutical market, including the GLP-1 receptor agonists currently generating tens of billions in revenue, is treating a symptom of the same unmanaged program. [The only weight you gain from beginning to end is fluids and electrolytes. Once you convert, you establish a reset point to which you will return during the phase transitions]
Addiction susceptibility reduction. The organism has documented access to every major reward and reinforcement pathway: dopaminergic signaling (Gpr1), endocannabinoid tone (arachidonic acid competition, CB1 density maintenance), serotonergic regulation (tryptophan diversion to kynurenine), and GABA interactions. Alcohol is a direct fermentation product and substrate — the organism produces ethanol endogenously. In a managed state, reward pathway modulation produces a stable hedonic tone. In an unmanaged state, it produces the depleted, dysregulated reward landscape that drives self-medication and compulsive substance use. The $740 billion annual cost of substance abuse in the United States includes the cost of humans attempting to restore neurochemical balance that the organism has disrupted. Managed oscillation intervals restore that balance at the source.
Longevity – [Lazarus Long]
The organism’s program is not designed to kill the host. It is designed to maintain the host. Every maintenance subroutine — cholesterol management, glucose regulation, immune calibration, cardiovascular governance, infection suppression — exists because the organism benefits from a living, functioning host. The organism has no evolutionary incentive to accelerate host death. It has every incentive to delay it.
Homo Candidus goes through a precise sequence of events over decades. The organism will literally do everything within its power to keep you alive in the Homo Candidus state [this cannot be said for Homo Sapiens]. It will not let you die if it can prevent it, and if you doubt that, then you should read this case report**:** Acute Hemodynamic Decompensation Following Routine Phlebotomy in a Patient with Chronic Volume Dysregulation: A Five-Week Longitudinal Provocation Sequence (Craddock ,2026d). This author has survived 30 years in this state with a medical system that was oblivious to the condition and had no idea what was going on [despite thinking the contrary]. The number of times I would have died had I not been Homo Candidus is more than a few, with the first one in 1995, triggered by antibiotics prescribed for a UTI that wasn’t there. Instead, I had an organism already managing my urinary sphincter and ADH mechanisms, and I was prescribed two different antibiotics and a barbiturate in rapid succession and went into SIADH [and a whole lot more – push the button harder each time].
The conditions that currently limit human lifespan in developed nations — cardiovascular disease, cancer, metabolic disease, neurodegeneration — are, within this framework, consequences of unmanaged program advancement. They occur because the organism’s colonization density and program state reach levels that overwhelm the host’s compensatory capacity. They are not inevitable features of aging. They are features of unmanaged coevolution.
If the phase intervals (Redacted Science, Craddock 2025) can be maintained — if the organism’s program is periodically reset before it reaches the density at which pathological outputs overwhelm maintenance functions — then the host remains in the managed maintenance state indefinitely. The organism continues to manage cholesterol, regulate glucose, suppress infection, calibrate immune function, and govern cardiovascular tone. The host does not develop the progressive organ system failures that currently define the aging trajectory.
This is not a speculative claim. It is a mechanical consequence of the framework. If the organism is performing maintenance, and the maintenance is periodically renewed, then the systems being maintained do not degrade on the timeline they currently follow.
The billionaire longevity industry — the tens of billions being invested in senolytics, NAD+ precursors, rapamycin analogs, telomere extension, and caloric restriction mimetics — is searching for the mechanism that prevents the progressive deterioration of human organ systems. The framework described in this series proposes that the mechanism already exists. It has been running for over a million years. It is not a drug. It is not a gene therapy. It is a relationship that humanity forgot it had. It can be activated.
The practical ceiling on managed human lifespan cannot be stated with precision because no controlled data exist. But the trajectory is clear. Current human life expectancy in developed nations averages approximately 80 years under conditions of complete ignorance about the organism’s role — conditions in which every chronic disease it produces is treated as a separate problem, every metabolic parameter it manages is medicated independently, and every organ system failure it drives is addressed only after it manifests. If even a fraction of the organism-mediated decline described in this framework is preventable through managed phase transitions, the implications for human lifespan are measured not in years but in decades. Focusing all the research money in this area would create a tsunami of advancement.
Technology accelerates this. AI-driven diagnostics can identify colonization density and program state markers that no human clinician currently looks for. Precision medicine can optimize oscillation intervals for individual physiology. Genomic analysis of the organism’s 1,300 uncharacterized orphan genes will reveal maintenance functions that 200 million years of coevolution have refined but that science has never examined.
The Shift
The United States currently spends $5.3 trillion per year on sick care — on managing the downstream consequences of a relationship it does not know exists. That figure is projected to reach $8.6 trillion by 2033. Chronic disease alone will cost $47 trillion over the next fifteen years. This trajectory is unsustainable by every metric available, and every proposed solution — value-based care, preventive screening, pharmaceutical innovation, lifestyle intervention — operates within the same paradigm of treating symptoms produced by systems whose upstream governance has never been examined.
The framework described in this series does not propose an incremental improvement. It proposes a paradigm shift of the kind that restructures entire fields. The germ theory of disease did not improve humoral medicine. It replaced it. The recognition that a managed coevolutionary relationship underlies the majority of chronic disease in the developed world does not improve the current model of treating each condition as an independent entity with its own pharmaceutical pipeline. It replaces it.
The implications extend beyond lifespan. A managed Homo Candidus phenotype means a population without epidemic obesity, without the psychiatric burden that currently disables tens of millions, without the autoimmune diseases that disproportionately destroy women in their most productive years, without the addiction cycle that consumes $740 billion annually and tears apart families and communities, without the metabolic deterioration that medicine currently treats as an inevitable feature of aging. It means children who do not develop the neurodevelopmental and behavioral conditions that are increasing in prevalence with every generation. It means a healthcare system that actually promotes health rather than managing an endless cascade of symptoms produced by a relationship no one knew existed.
The longevity revolution that every futurist, every biotech investor, and every AI-driven health platform is predicting — the shift from 80-year lifespans to 120 and beyond — is not going to come from a new drug. It is going to come from understanding what has been managing human physiology for over a million years and learning to work with it instead of against it. Or, more precisely, instead of not knowing it exists at all.
This is not the first time the thread was found. In the 1960s, a UK research corridor converging on the same organism-host relationship was dismantled, its researchers marginalized, and its findings buried under reclassification and institutional silence (Craddock, 2026e). That suppression cost sixty years. The difference now is that the data are published, the framework is citable, and the archive is distributed beyond the reach of any single institution. It cannot be thrown away again.
[This is it, and it was here all along waiting for us to notice, again]
A Note from the Architect
Is this condition perfect? No. Is it measurably better? Yes, it is better for both individuals and society.
We face a choice – keep trying to kill our regulatory symbiote and increasing the number of diseases and pushing pills in their direction that really talk to the organism on side channels we are not examining, or embrace it and stop spending trillions of dollars on diseases of our own creation.
Ultimately, the decision is up to you. I’ve had my ride on the merry-go-round. I did it with no safety net – not one physician thought I was any different than any other average human being in a substantial way. I made it more than 30 years from the date I converted, and trust me, I made mistakes along the way that cost me at least a decade, by my estimates. Add just 5 years to 3 stages, and you make it 45 years (easily age 75 and healthy almost every day of it). Add 10, and you accomplish 60 (easily age 90). The science will be focused and well-funded. I would expect greater improvements. I do not know the limits, but they are much greater than the direction we are currently headed.
[Your Symbiont would like you to share]
Write a comment